Dear Dr Quinn:
My 19-year-old daughter was diagnosed with AD/HD last June. She left for college with Adderall and came home four months later, with a GPA of 4.0 in Biochemistry and a major case of depression, and lots of anxiety. She was extremely irritable all semester. To make a long story short, after four (4) different antidepressants, and three months with her psychiatrist, she has been diagnosed with Bipolar Disorder. She went into a hypomania state after the fourth antidepressant was started. Needless to say, I am devastated and sad, but glad to know that the “something” that has been wrong for so long has a name. She has been taking Lamictal for five days. I am hoping that this Mood Stabilizer will be an answer for her.
Do you have any info or web page that deals with ADHD/Bipolar? I have been reading Driven to Distraction (which my daughter has read), Bipolar Disorder for Patients and Their Families, Stop Walking on Egg Shells, and An Unquiet Mind (Kate Jamison is my new hero). My daughter is reading her book, too. She is on medical leave this semester and the goal is to get her healthy enough to work at the beach this summer and to return to school next fall. Right now, she cannot work at all, but does seem much less depressed and the hypomanic mode is gone. Thanks so much.
Lyn
Dear Lyn:
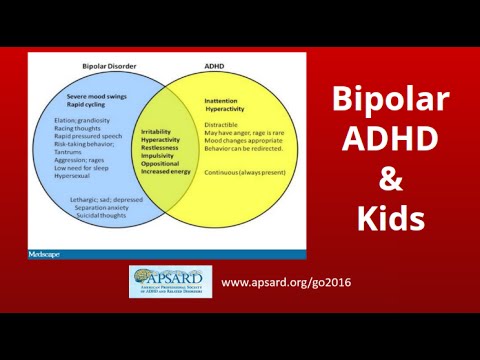
It sounds like your daughter is receiving excellent care. AD/HD and co-existing Bipolar Disorder (BPD) is extremely common. The one comment I would add about her treatment regards her AD/HD diagnosis. So often, treatment of AD/HD falls by the wayside as Bipolar is treated, and the AD/HD symptoms continue to impair functioning.
Once mood is stabilized for those with AD/HD and Bipolar Disorder, a low dose of long-acting stimulant should also be considered in order to optimize functioning. You might want to read more about this on our website in an article by Dr Bill Dodson. He also has a chapter on “AD/HD and Bipolar Disorder in Women” in our book, Gender Issues and ADHD.
A recent report addressing this issue has recently been published. * Two studies from researchers at Massachusetts General Hospital (MGH) discuss the challenges of diagnosing and treating individuals with both attention-deficit hyperactivity disorder (AD/HD) and Bipolar Disorder (BPD). Published in the July, 2003, issue of Biological Psychiatry, one report clearly identifies symptoms of both disorders in study participants, supporting the theory that some individuals truly suffer from both disorders. The second study in the same issue finds that the antidepressant bupropion (Wellbutrin) may be helpful in treating those with both AD/HD and BPD.
“The question of whether ADHD and BPD can exist together has been controversial, with some believing that such diagnoses reflected particularly bad ADHD or that the manic symptoms of bipolarity were simple hyperactivity,” says Timothy Wilens, MD, of the MGH Pediatric Psychopharmacology Unit, lead author of both papers. The first study tells us these are distinct disorders that can occur and be identified in adults. “Treating adults with ADHD and BPD has been difficult because the stimulants and many other medications used for ADHD may exacerbate manic symptoms,” he continues. “However, not addressing both disorders in these individuals can make their lives more difficult.”
In the first study, adult patients who had come to the MGH to participate in ADHD clinical trials went through an extensive clinical assessment of psychiatric symptoms. This included a complete medical history, psychiatric evaluation, a diagnostic interview with a section addressing ADHD, and tests of cognitive function. Data from the diagnostic interview were subsequently reviewed by a team of mental health professionals who were not informed of the patients’ diagnoses, to confirm whether the symptoms reported made a significant difference in patients’ functioning.
Of those evaluated for this study, 51 met full criteria for ADHD diagnosis, and 24 also met established criteria for BPD. Along with their BPD symptoms, participants with both disorders had a greater number of ADHD symptoms than those with ADHD alone, and 60 percent of those with both disorders reported having BPD symptoms starting at a young age. Both groups also had additional psychiatric disorders, but those with both conditions had a higher risk of additional disorders.
“Although the hyperactive/impulsive symptoms of ADHD tend to lessen as patients mature, it appears that those who also have BPD continue with those symptoms as adults. So if a youngster with ADHD continues to have prominent hyperactivity and impulsivity while growing up, it may indicate that accompanying BPD should be considered,” Wilens says.
Bupropion — an atypical antidepressant — was chosen for the second study because it already is used to treat individuals with ADHD and to treat depressive symptoms in BPD. During the six-week study period, 30 participants diagnosed with both disorders began taking a daily 100 mg. dose of bupropion and increased their dosage to a maximum of 200 mg given twice daily. Any participant who felt that a particular dosage provided superior symptom relief could return to that dosage. Most of the study participants showed significant improvement in their symptoms of both disorders, with 70 percent reporting that symptoms were “much improved” or “very much improved.” A majority of study participants continued taking the medication at the conclusion of the study.
“I have evaluated and followed a number of those participating in this study,” Wilens says, “and they have noted major life changes associated with their improved functioning and well being. Many went from being incapacitated and unable to sustain relationships to being employed and reporting improved relationships and overall well being.” Wilens is an Associate Professor of Psychiatry at Harvard Medical School. He and his colleagues note, however, that because of this study’s small size, along with the facts that there was no control group and all participants knew the dosages they were receiving, additional large-scale controlled trials are necessary.
Both studies were supported by grants from the National Institutes of Health. The bupropion study also received support from GlaxoSmithKline, Inc., manufacturer of the Wellbutrin brand of bupropion. However, the MGH researchers had complete control of the study design and reporting. Wilens’ co-authors for the first study are Joseph Biederman, MD, Janet Wozniak, MD, Samantha Gunawardene, Jocelyn Wong, and Michael Monuteaux. The second study was co-authored by Biederman, Jefferson Prince, MD, Thomas Spencer, MD, Stephaine Van Patten, Robert Doyle, MD, DDS, Kristine Girard, MD, Paul Hammerness, MD, Sarah Goldman, and Sarah Brown.